


THREE doctors, TWO countries, ONE enemy
They may have come to New York at diverse times and with various aspirations, but as the pandemic arrived, their Chinese backgrounds gave them a unique perspective as they joined in battle against the virus.











Zhang Jin, a Chinese American doctor, remembers the day when the urgent care clinic in which she works in Flushing, New York, was swamped by patients showing symptoms related to COVID-19.
"It was March 18, and people seemed to have come out of nowhere," she says.
Barely a week later New York was experiencing a surge of confirmed cases, followed by a rising number of deaths every day, with a peak of about 800 one day in April.
"If we could possibly go back to that day, I would say to anyone willing to listen: test as much as possible; get treatment as early as possible," Zhang says.
Over three months Zhang found herself face-to-face with more than 100 people who had contracted COVID-19.
"We couldn't test any patient until March 24, when a laboratory told us they could take our samples. I sent out six samples in the first week and eight in the second, although I knew that the overwhelming majority of those who came to us would have the virus.
"It was impossible to have everybody tested because the laboratories were inundated with test requests, including from hospitals treating only those with severe symptoms, and we didn't want to divert attention from them."
Someone who did get a test early on was Pang Peng, a psychiatrist at Staten Island University Hospital. She has been providing psychological counseling and support to COVID-19 patients, their family members and doctors, both in the hospital and at home by phone.
She realized she had a fever and chill on March 14 and decided to get tested.
"The hospital was then sending out only two to five test samples each day," said Pang who, when symptoms appeared, immediately called Zhang, who with her husband studied medicine in China.
Over the next few days Pang's condition deteriorated, her oxygen saturation falling sharply, meaning that just to ensure relatively smooth breathing she needed to sit up slightly.
"I first went to the hospital but later decided to stay at home, partly because at the time US hospitals had little experience in treating COVID-19 patients. At one point I was lying on a bed as my husband patted my back until I coughed up a thick blob of sputum."
Over those days Pang's condition ebbed and flowed, and she relied on an oximeter to monitor her condition. For her the palm-sized device was a godsend, the very last one a local pharmacy had had in stock. It is clipped onto one's finger and measures oxygen levels in red blood cells, a normal reading being between 100 and 95. Pang's dropped to as low as 85.
"Since COVID-19 patients with mild symptoms are required to stay at home in the US, self-monitoring is crucial, especially for those with COPD," says Pang, referring to chronic obstructive pulmonary disease, an inflammatory condition that obstructs airflow from the lung.
"Usually, healthy people whose blood oxygen reading falls below 88 percent find it hard to breathe and immediately need to go to hospital to have a nasal oxygen tube inserted, which helps alleviate symptoms while their condition is being monitored.
"It's not uncommon for somebody with COPD to have a much lower oximeter reading, even if they don't have COVID-19. These people may have got used to compromised breathing, but they are at grave risk."
With COVID-19, those who are obese or have high blood pressure or diabetes are also regarded as highly vulnerable. Such conditions can impair the microvascular system, leaving the person prone to clotting once COVID-19 infection triggers inflammation.
Oximeters that can help sound the alarm had largely disappeared from pharmacy shelves by mid-March.
At the height of the pandemic in April, a video on the internet showed a tearful New York doctor lamenting patients being delivered in ambulances to hospitals when it was too late, because they were dead.
Jiang Shasha, an intensive care doctor with Northwell Health in Queens, New York, said: "I saw a young man whose blood oxygen reading had plummeted from 90 to 60 percent within half an hour, before he suffered a cardiac arrest and died.
"We call it Code Blue," says Zhang, referring to an emergency situation when a patient's blood oxygen level plunges, leaving him or her close to death.
Apart from self-monitoring, Zhang sees "early supportive care" as essential in improving a patient's chance of beating COVID-19.
"The whole purpose of supportive care is to make patients feel more comfortable-no high fever, no severe coughing, no dehydration-so they are better placed for the gradual release of their own immune power," she says.
"There's no medication to fight the virus directly, but some drugs can slow down viral replication and give the immunity system the chance to begin restoring itself."
One such drug Zhang has been giving to her patients is hydroxychloroquine, whose effectiveness and possible side effects are a matter of strong contention. The drug, routinely used to prevent or treat malaria, has been found to make cells less hospitable for viruses, and there have been hopes that it could do the same to coronavirus-2(SARSCoV-2) that causes the disease now called COVID-19.
Another type of medicine Zhang has resorted to is antibiotics.
"Technically, you don't need antibiotics to combat a virus. But COVID-19 weakens one's immune system, making the patient more susceptible for a bacterial infection, bacterial pneumonia for example which aggravates the situation. That's why we need antibiotics," she says.
But not everyone agrees with this approach, says Pang.
"Some US doctors may opt to give antibiotics to patients with weaker immune systems-old people, for example-but most would be reluctant to dispense it to young patients with no apparent underlying problems," she said.
Reflecting on the controversy surrounding certain medicines, Pang believes that the knowledge gained about a medicine is inevitably shaped by the circumstances under which it is administered.
"Here in the US, with rare exceptions, most COVID-19 patients have received hydroxychloroquine and chloroquine in the hospital, when their condition has become serious enough for them to be admitted. Therefore, the conclusion that a medicine has little effect may hold more truth for a specific group of people, instead of all who are infected."
David Ho, one of the leading AIDS researchers and virologists in the United States, best known for his therapy combining multiple medications that enhance and complement one another, says the same approach would work for COVID-19. Patients should be treated with this approach at the onset of symptoms, not later, he says.
But only if the reality on the ground would allow for that.
"Take hydroxychloroquine for example," Jiang the ICU doctor says. "We did notice that the drugs had little positive effect on our most severe patients. But what could we do? We were short of drugs and could not possibly give them to everyone in need, including those for whom the drugs may hold greater promise. At the end of the day the most critical patients were still our top priority."
Jiang lives in Queens, New York, a borough populated by working class and immigrant families, and has some of the areas the pandemic has hit hardest.
"One day in April the building's plumber, who comes from Costa Rica, came to my room to do some repairs. He told me that many people in our building had been infected, resulting in multiple deaths within one family.
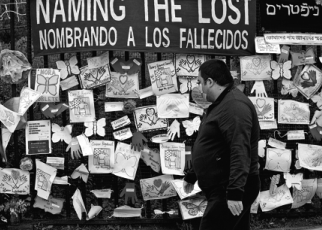
"One time he saw several black body bags being carried out in quick succession from one apartment. There was a 108-year-old woman who had survived the Holocaust but died of COVID-19, a few days before her son, in his 60s, died. Her arm carried a serial number, a painful reminder of being a prisoner in a Nazi concentration camp."
Lack of effective quarantine caused the disease to spread, especially among people who lived with others in cramped spaces. Between mid-March and late April the sharp rise in infections was acutely felt, nowhere else more so than in the hospitals.
"Every morning I had to literally drag myself out of bed," Pang says.
"My body felt leaden, not because of exhaustion but because of sadness and helplessness that kept sinking into me."
Pang, who as a psychiatrist liaises between patients and their families and physicians, tells of a patient who needed to have a leg amputated because of severe clotting.
"Post-operation, his condition stabilized-at least we all believed so. We called his family to tell them of the progress, only to come back the next morning to find him gone forever.
"I've seen so many lives come to an abrupt end, so I've learned to rein in hope, if only to save the family from total devastation. But a certain part of me always longs for one good piece of news."
Pang studied at the Peking University Health Science Center in Beijing before coming to the US in 1993 and remains an active member of her former circle. She was back in Beijing on Jan 22, two days before Chinese Lunar New Year's Eve, and one day before the lockdown of Wuhan, where the battle against a mysterious and fast-spreading virus had begun.
By the time Pang left Beijing for New York on Jan 30, twenty doctors from the Peking University First Hospital, affiliated with Pang's alma mater, were already in Wuhan, joining other medical teams from across China. Two designated COVID-19 hospitals, with a total of 2,600 beds, were half way through being builtin a lightning-fast 10 days or so.
For the next month Pang updated herself on all COVID-related news from China, searching and buying personal protective equipment to be sent to frontline doctors in the country.
On Jan 24 she joined a volunteer group consisting of licensed psychiatrists, psychologists, social workers and nurses in North America, all with a Chinese background. From then until early April through a messaging app they provided psychological consultation and peer support to frontline doctors and nurses in Wuhan.
Pang was to find a striking similarity between her own tribulations and sadness and of those she had sought to relieve.
"Some lament what is seen as a lack of communication between the US and China in dealing with this global issue. In fact, exchanges between medical professionals on both sides have been going on since January, much facilitated by Chinese doctors who are here on exchange programs, and by those who once pursued their Political and cultural differences have often been cited by people trying to understand the situation. As a doctor, Zhang is keenly aware of constraints inherent in the country's medical system.
"In the US the entire medical system is structured in a way where a patient is first supposed to go to his or her primary care doctors or urgent care doctors as in the case of an emergency. From there they are referred to specialists operating either from their own clinics or in big hospitals, for further examination and any medical procedures. The COVID-19 onslaught ripped through that chain."
The US Centers for Disease Control and Prevention has recommended that people "go to see your doctor" at the appearance of COVID-19 symptoms. But by mid-March most primary care doctors in New York had closed their clinics, although some had switched to telemedicine.
Every week Zhang spent three days in her own primary care clinic in Flushing and another one or two days in the HealthNeed Medical Urgent Care, where she met most of her COVID-19 patients.
"Almost all urgent cares have remained open, but you cannot stop staff from resigning, like many working at the front desk of New York urgent care centers did. You can't blame them. Across New York, health care professionals were becoming infected in unprecedented numbers."
Zhang decries the fact that early on President Donald Trump made light of the seriousness of COVID-19, comparing it with the flu.
"It was highly misleading and has had a lasting impact on people's perception of the disease."
She also disagrees strongly with what she sees as the Trump administration and some state governments discouraging people from taking tests and seeking early treatment.
When Tian Liyan, 74, in New York on a visitor visa, called the public hotline on April 18 to inquire about tests, she was already one week into her sickness.
"I was told to stay at home as long as my condition was stable, since 'tests are performed only for people who are having severe symptoms like high fever or breathing difficulty and therefore have been admitted'," she says.
"Since I was in New York visiting my family I obviously needed to know whether I was infected so I went to Elmhurst Hospital. There were three doctors and only one patient, and anyone who wanted a test could get it right away."
Two days after her test, Tian felt that her condition had deteriorated, but not so much that she could be admitted to the hospital. Through a mutual friend, she called Zhang, who told her immediately to visit a nearby urgent care center, where she was X-rayed.
"The doctor told me there was no need to wait for the test result because the picture showed an opaque lung. … The test result came out three days later."
Jiang says that in the early days of the Wuhan outbreak, when test kits were scarce and results were not totally reliable, China's National Health Commission listed medical imaging as one of two methods (the other being the test) that could lead to a positive diagnosis and therefore ensure being given a hospital bed.
This practice continued until the test was no longer a big issue in quantity and accuracy.
"In New York no machines are solely reserved for COVID-19 patients and the patients are not typically given a CT scan before they are admitted into the hospital," Jiang says.
"Do not test patients if your treatment plan is not going to change based on the test result" was the message from the CDC to US doctors, who, Zhang says, did not always see eye to eye.
"I've met several doctors who do not quite believe in aggressive early medical intervention. To stay home, drink a lot of water, eat fruit and take anti-fever medicine when it's necessary-that's all they suggest, not that different to what you're expected to do when contracting a flu."
Yet all three doctors agree that the utter unpreparedness in which the US found itself in March, when infection numbers took off, left doctors and patients with few options.
News reports in mid-March described people lining up in the rain for at least a day to get a test at Elmhurst Hospital in Queens, the hospital Tian Liyan went to.
Elsewhere, Flushing Hospital Medical Center, with its 293 beds, had more than 600 in-patients at one time. Even storage space was occupied by medical beds.
"Tests as well as urgent-care centers and emergency departments were not recommended then for mild cases or young people, because they didn't have capacity to handle that vast number of people," Pang says. "If people all went, there would simply be more cross-infections and possibly more deaths."
"The situation with the mask and oximeter was probably the same-how could the government recommend it if they could not make it available to everyone in need?" she says.
The doctor says she was well aware of it when community-acquired COVID-19 infections started spreading on Staten Island, where she lives and works, in late February.
"Staten Island has a large European population, and there was a lot of travel during the holiday season. Chances are that some brought the virus back with them when they returned from Europe."
By the end of May, Jiang had her antibody test in her own hospital and the result was "equivocal", meaning she was mildly or borderline positive. "There are two possibilities. First, at the time of the test, I had just become infected and had yet to develop very strong antibodies; second, I was infected months ago and had since recovered, with the antibody turning weaker and weaker."
The first time Jiang had a test was in mid-March, after being exposed to her hospital's first confirmed COVID-19 patient. It was a nucleic acid amplification test using a nasal swab specimen. The result was negative and she could not get a second test.
"The patient was tested on March 9 and the result came back two days later. Before him, the hospital had no testing right, which meant that although we have a large laboratory, the hospital had to apply to the New York State Department of Health if we wanted to test a suspected case. As a result, some died in early March before they could be tested."
On March 18, seeing so many patients around her gave Zhang a mental jolt, and her first reaction was to reach out for a mask. "The medical assistants at our front desk were still wearing loose-fitting surgical masks that can do nothing to block the tiny particles carrying coronavirus. At my suggestion they borrowed a box of N95 from a gastrologist upstairs. I put on the mask and gown, took a picture of myself and used it as my WeChat avatar, which it still is."
Pang says the first day that doctors were required to wear masks in all areas of her hospital was March 13, one day before she became ill.
"Exactly a week earlier we wore masks only in emergency rooms."
Between her own recovery in early April and mid-May, when daily death numbers consistently fell in New York, Pang spent most of her day with patients, some in intensive care.
"People straddling the line between life and death are clinging on desperately to hope, and need mental support as much as they do air. We were all out there for them-the hospital's entire team of psychiatrists."
Every night she was at home counseling and comforting resident doctors in her own hospital, sometimes late into the night.
"They are mostly in their late 20s and early 30s and haven't seen the worst of times. Some cried as we talked. I understand every bit of their fear and their emotions, which only makes me want to salute their heroism more.
"No matter what we have been through, when it's time to say goodbye for one last time we will say it with the patient's hand in our hands."













Today's Top News
- Philippines' baseline claims riddled with legal holes
- Bruce Lee's enduring legacy of adaptability
- Dancing to the rhythm of culture and tradition
- Evolving beyond friction to harmony
- PLA's airborne nuclear strike system shown
- Kinship, roots link Chinese at home, afar








